Christopher J. Webb, United States
Fellow
Kidney and Pancreas Transplant
Atrium Health Wake Forest Baptist
Does dialysis modality or duration influence outcomes in simultaneous pancreas-kidney transplant recipients in the modern era?
Christopher J Webb1, Colleen L Jay1, Matthew Garner1, Alan C Farney1, Emily McCracken1, Robert Stratta1, Giuseppe Orlando1.
1Surgery, Atrium Health Wake Forest Baptist, Winston-Salem, NC, United States
Introduction: The influence of dialysis modality and duration on outcomes following simultaneous pancreas-kidney transplantation (SPKT) remains uncertain in the modern era. Methods: We performed a single-center retrospective review in 255 consecutive SPKT recipients according to terminal dialysis modality (55 preemptive/no dialysis-ND, 70 peritoneal dialysis–PD, and 130 hemodialysis–HD) and duration (55 ND, 137 <2 years, 41 2-4 years, and 22 >4 years on dialysis). We also performed a sensitivity analysis for patients who had any exposure to PD (55 ND, 88 PD ever, and 112 HD only).
Results: Mean follow-up was 9.4 years (median 9.2 years). The early (3-month) relaparotomy rate (20% ND vs 36% PD/HD, p=0.03) was lower in ND patients. There were no differences in early graft loss, patient survival, overall or death-censored kidney or pancreas graft survival rates (GSRs) at 1 or 10 years follow-up according to dialysis modality. When analyzing dialysis duration, there were no differences in rates of pancreas thrombosis or early pancreas graft loss. Kidney delayed graft function (DGF) was lower in the ND/short dialysis groups combined (1.0%), compared to the intermediate/long dialysis groups combined (9.5%, p=0.003). Early relaparotomy rates were higher with longer duration of dialysis (p=0.045 between ND and >4 years of dialysis). Patient survival in the long dialysis group was 50%, compared to 69.5% in the other three groups combined.
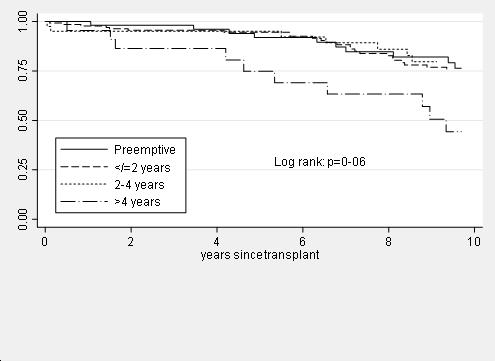
However, both overall and death-censored kidney and pancreas GSRs were comparable according to dialysis duration. In a Cox regression analysis of patient survival, dialysis duration >4 years and older recipient age were the only significant variables associated with diminished patient survival both in the univariate and multivariate models. Absence of dialysis, dialysis modality and dialysis duration did not affect either kidney or pancreas GSRs in the univariate and multivariate models. Findings were similar both in the standard and sensitivity analyses, which reclassified 18 patients into the "PD ever" category. In a logistic regression analysis for early relaparotomy, dialysis duration <2 years or >4 years and longer pancreas cold ischemia were significant variables affecting the risk of early relaparotomy.
Conclusions: Preemptively transplanted patients had a lower incidence of kidney DGF and early relaparotomy whereas patient survival was slightly lower with longer dialysis vintage prior to SPKT. Dialysis modality and duration did not influence either overall or death-censored pancreas or kidney GSRs in the setting of short waiting times, low Kidney Donor Profile Index donor organs, and dialysis duration up to 4 years.