Islet isolations from extended criteria donors
Alan Timpson1, Caroline Fattah1, Lora Irvine1.
1TCAT, SNBTS, Edinburgh, United Kingdom
Introduction: Organ utilisation is a significant issue regarding donation of human pancreata. The current pancreata donor acceptance criteria applied by most UK islet isolation centres for donation after brain stem death (DBD) and donation after cardiac death (DCD) are summarised below.
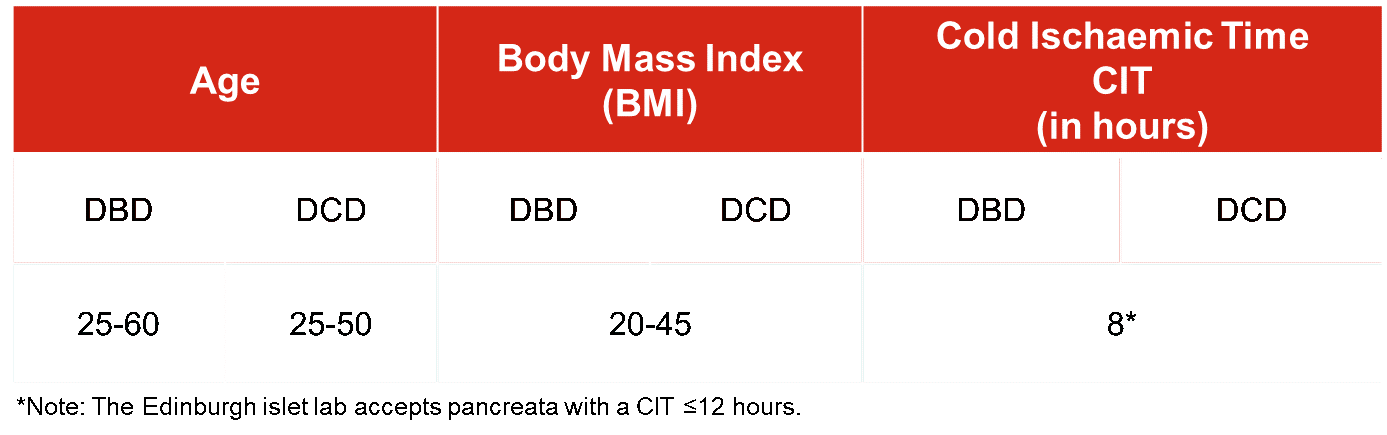
These parameters restrict organ utilisation. This study aims to assess the following extensions to the acceptance criteria on islet isolation outcome; 1. Effect of increasing CIT from ≤8 hours to 8-12 hours and >12 hours; 2. Effect of extending the criteria to include donors <25 year old.
Methods: Isolation data for pancreata with CIT ≤8 hours were compared to 8-12 hours CIT. Pancreata with CIT >12 hours were accepted as a second extension and released under concession. The acceptance criteria was further extended to include donors <25 years old with a CIT of ≤12 hours. All pancreata underwent clinical islet isolation. A successful outcome was determined by whether the final islet cell product met the release criteria (yield ≥200000 islet equivalents (I.Es), viability ≥70 % and purity of ≥30 %) and if it proceeded to transplant.
Results: The majority of pancreata accepted by the Edinburgh islet lab (64 %) fall within an 8-12 hour CIT. The outcome of these isolations were comparable to those from pancreata with a CIT of ≤8 hours. The average yields for ≤8 hour CIT were 249864 ±141272 (n= 91) compared to 264658 ±171566 (n= 208) for a CIT of 8-12 hours. In the ≤8 hour CIT group, 56 % of isolations met the release criteria and 35 % of isolations proceeded to transplant. For the 8-12 hour CIT groups, 60 % met the release criteria and 40 % were transplanted.
Isolations were carried out in 21 pancreata from donors <25 years old. These were split into BMI <25 (n= 8) and BMI ≥25 (n= 13) groups. In the BMI <25 group, 1 (12.5 %) isolation met the release criteria with none progressing to transplant. However, in the BMI ≥25 group, 10 isolations (77 %) met the release criteria and 9 (69 %) progressed to transplant. Follow-up data demonstrated that 75 % of patients who received these transplants were insulin independent for 1-4 years post-transplant; higher than the national average of 17 %.
At >12 hours CIT, average yields dropped to 211477 ±171147 I.Es, with 40 % of isolations meeting the release criteria and a transplant rate of 24 % (n= 25).
Conclusions: No detriment to isolation outcome was observed when pancreata CIT is increased from ≤8 hours to 8-12 hours. Isolations in pancreata from donors <25 years old with a BMI ≥25 demonstrated above average outcomes when measured by isolation success and transplant rate. Furthermore, there is evidence to suggest an increased rate of insulin independence in patients who receive transplants from this subset.
Therefore, extending the acceptance criteria to include pancreata with CIT ≤12 hours and from younger donors with high BMI has the potential improve organ utilisation, thereby increasing the number of patients treated.



