Analysis of collagenase dose on allogeneic islet isolation outcomes and glucose-stimulated insulin release
Doug O'Gorman1, Tatsuya Kin1, Shawn Rosichuk1, Wendy Zhai1, Jennifer Moriarty1, Kyle Park1, Advaita Ganguly1, Peter A Senior1,2,3, James AM Shapiro1,2,3.
1Clinical Islet Transplant Program, University of Alberta, Edmonton, AB, Canada; 2Department of Surgery, University of Alberta, Edmonton, AB, Canada; 3Alberta Diabetes Institute, University of Alberta , Edmonton, AB, Canada
Introduction: The use of a low collagenase dose has been previously reported as potentially being beneficial to allogeneic islet isolation outcomes and specifically the glucose-stimulated insulin response (GSIR). In this study, the effect of the low collagenase dose on islet isolation and insulin secretion is expanded to investigate the role of the enzyme type and non-collagenolytic components.
Methods: Clinical islet isolations were performed utilizing standard-of-care protocols between Jul 2008 and Mar 2023. Pancreases were perfused with an enzyme blend of either a non-targeted Liberase MTF high collagenase dose with thermolysin (HD-MTF, n= 441), a targeted (<20 WU/g) Liberase MTF low collagenase dose with thermolysin (LD-MTF, n=41) or a targeted (<20 WU/g) rCollagenase HI with BP Protease low collagenase dose (LD-rHI, n=93). Dynamic GSIR testing was performed at the time of the islet transplant using approximately 100 IE. Islets were exposed to 16 min intervals of low glucose (2.3 mMol) and high glucose (23.0 mMol) following a 60 min stabilization period. Perfusate was collected and analyzed for insulin concentrations. Perifusion samples were collected, and islets were stained with dithizone, and quantified to normalize the raw insulin values. Stimulation indexes are reported as both peak to baseline as well as the area under the curve. Basal and stimulated metabolic rates were calculated to express the final islet product insulin secretion.
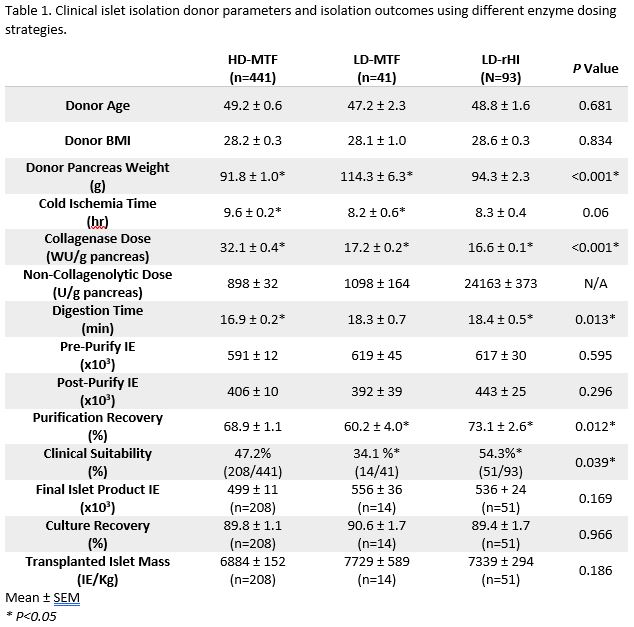
Results: In comparing some critical donor parameters across all groups (Table 1), HD-MTF had a significantly longer cold ischemia time and smaller pancreas than LD-MTF. The use of LD-rHI had a notably higher purification recovery despite pre-purification trapped proportions being similar between groups. Islet yields at all time points of processing showed comparable results, however, LD-rHI had a higher percentage of islet preparations proceed to transplant than LD-MTF.
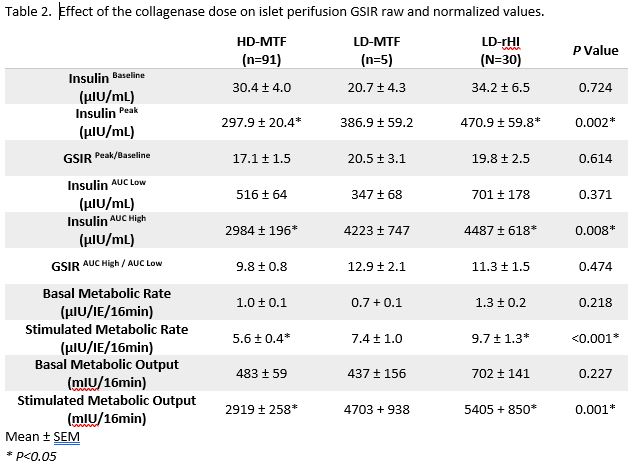
In assessing GSIR data (Table 2), the low-dose test groups both had higher stimulated responses to glucose than the high-dose control group, however, only the LD-rHI group was statistically higher. There was no observed difference between the 2 low dose groups. Both the raw and normalized stimulated insulin secretion levels were significantly higher in LD-rHI vs the HD-MTF.
Conclusions: The use of a low-dose collagenase is associated with improved islet isolation parameters as well as insulin secretion in response to high glucose and can effectively and reliably lead to improved islet isolation outcomes in comparison to the high-dose strategy. The results were similar when comparing the type of enzyme used with a low-dose protocol. However, there was an improved purification recovery and transplant success rate observed. Only the LD-rHI group showed statistical improvement on the standard high-dose approach when assessing insulin secretion. This could be a result of utilizing BP protease instead of Thermolysin as the non-collagenolytic component.



