Insulin independence with excellent glycemic control at 17-years post-islet alone transplantation: A case report
David Baidal1,2, Ana M Alvarez1, Camillo Ricordi1, Rodolfo Alejandro1,2.
1Diabetes Research Institute, University of Miami, Miami, FL, United States; 2Division of Endocrinology, Diabetes and Metabolism, Department of Medicine, Miller School of Medicine, University of Miami, Miami, FL, United States
Introduction: Although islet transplantation (ITx) can improve metabolic control in patients with type 1 diabetes (T1D), insulin independence is usually not sustained long-term. We describe the case of a female recipient with persistent insulin independence 17 years post-ITx.
Methods: A 50 y/o female with T1D of 20 years duration, weight 61.7Kg, BMI 21.3 kg/m2, insulin total daily dose (TDD) 0.29 units/Kg/day, HbA1c 7.8%, and normal renal function, underwent single-donor ITx (7,681 IEQ/Kg) with daclizumab induction and sirolimus+tacrolimus maintenance. Due to deterioration in glycemic control, a 2nd single-donor ITx (7,325 IEQ/Kg) was given 3.5 years after 1st ITx, with daclizumab+etanercept induction and same maintenance immunosuppression. Mixed meal tolerance tests, HbA1c, and insulin TDD were obtained at yearly visits. Continuous glucose monitoring (CGM) metrics over 14- days were obtained at last follow-up visit (Dexcom G6).
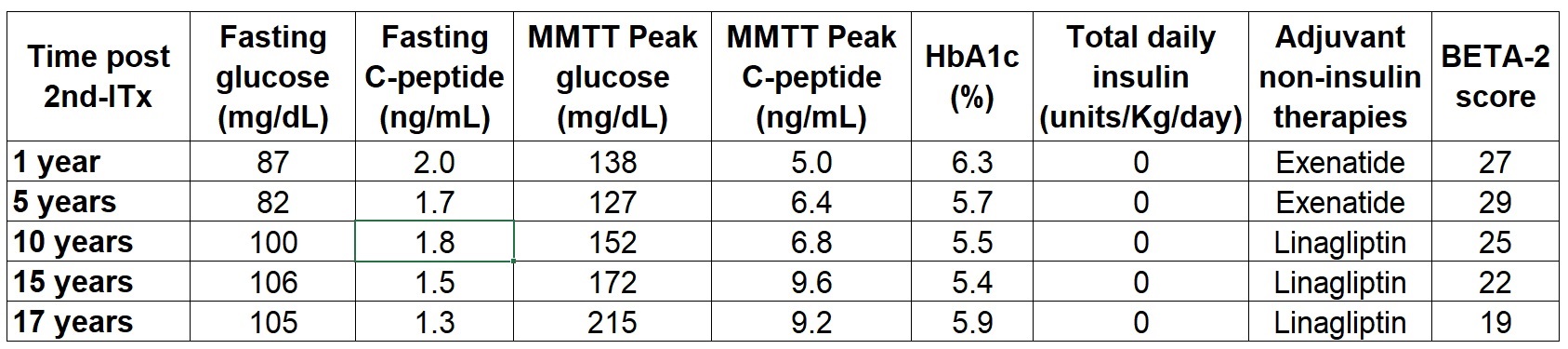
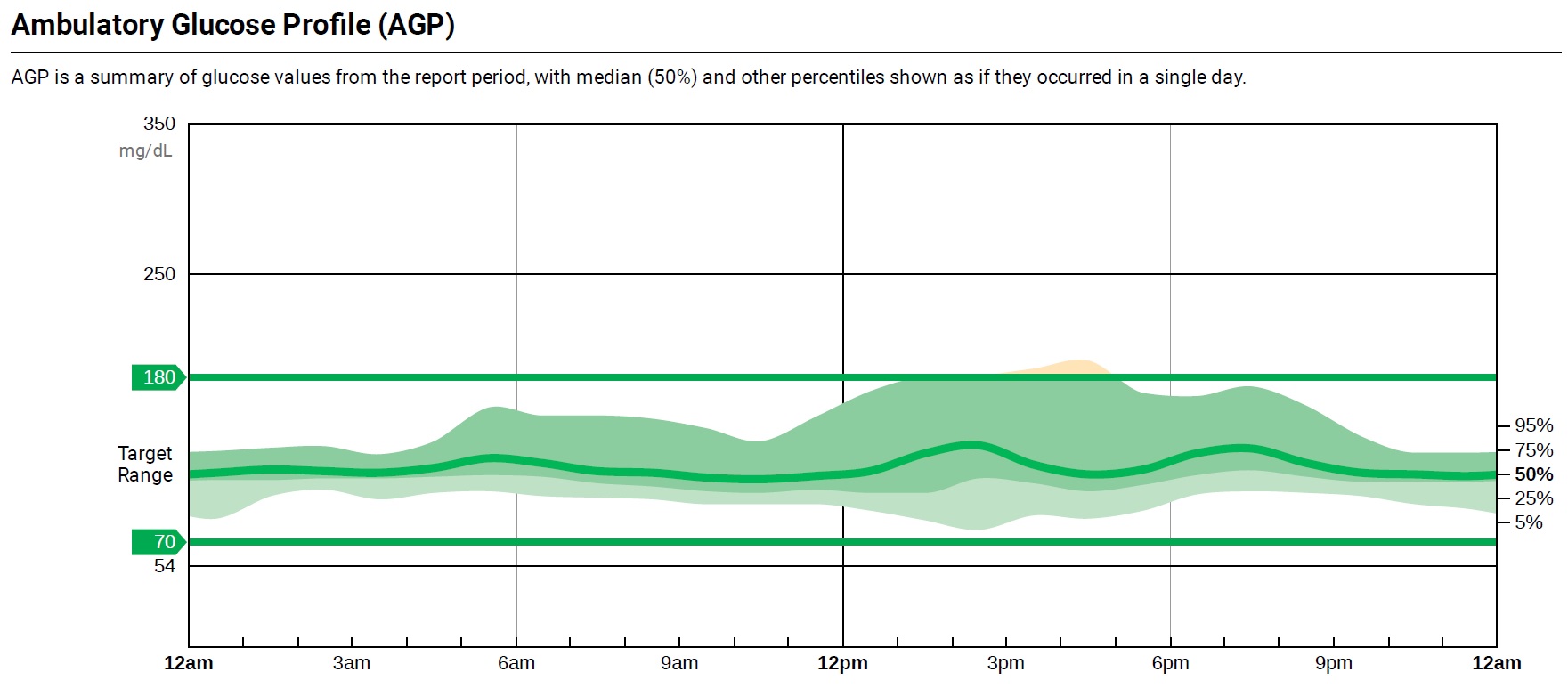
Results: Insulin independence was achieved 1-week post-1st ITx and was maintained for 23 months. To improve metabolic control, treatment with short-acting exenatide was started at 35 months. A 2nd ITx was given 40 months post-1st ITx. Prior to 2nd ITx, MMTT stimulated C-peptide was 3.8 ng/mL, insulin TDD 0.13 units/Kg/day, and HbA1c 6.6% (while on short-acting exenatide). The patient became insulin independent 9.5 months post-2nd ITx. At 5-yrs post-2nd ITx, exenatide was switched to liraglutide, and ultimately switched to linagliptin at 6.4-yrs. At 17-yrs post-2nd ITx, patient remains insulin independent with fasting glucose 105 mg/dL, MMTT stimulated C-peptide 9.16 ng/mL, HbA1c 5.9%, and BETA-2 score 19. CGM 14-days data review shows: time in range (70-180 mg/dL) 98%, time in range (70-140 mg/dL) 84%, time below range (<70 mg/dL) 0%, and CV 16.5%. MMTT data post-2nd ITx and CGM ambulatory glucose profile are shown in Table 1 and Figure 1.
Conclusion: ITx can maintain near normal metabolic control, evidenced by HbA1c and CGM metrics, for decades with complete abolishment of hypoglycemia. Identification of recipient and donor factors predictive of successful long-term ITx outcomes remains of critical importance to the field.